I’m desperately trying to get more free days to work full time while staying on home dialysis hd. But my nursing staff claim Medicare prohibits three times per week on the nxstage machine which is all I have available to me for use at home. I have spoken to Medicare and to other esrd organizations and patient advocacy groups and still no helpful information as to whether that is true or not. I’m just taking a final leap of faith and going around to ask patients if they’re aware of anyone doing home hemo three times per week or if Dr Agar or someone is aware of anything prohibiting patients from doing at home dialysis hd on the nxstage 3x/week.
IMPORTANT; my doctor already approved this schedule change and we worked out the necessary dialysis duration and dialysate volume in order to reach the standard required for ktv, but the center is saying it simply is not doable.
The Medicare Benefit Policy Manual, Chapter 11 on ESRD describes what Medicare will cover for HD and PD. The staff at your dialysis clinic are incorrect. Medicare routinely covers three HD treatments a week. Some patients use the NxStage machine to do extended (longer) dialysis sessions three times a week or every other day to get enough dialysis to feel well. Others use the NxStage machine to do nocturnal HD three nights a week while they sleep. When a patient does more than three dialysis sessions a week, it requires the doctor to medically justify the extra treatments. Although the clinic may prefer patients to do more treatments a week so they make more money if those treatments are Medicare approved, if your doctor orders three treatments a week, the clinic staff are required to follow the dialysis prescription. Here’s the Medicare manual I referred to. See Section 50 (page 33 of the PDF) for the information about the number of treatments Medicare will cover.
Thank you I will show this to them. This is similar to what I have been seeing in my own minimal research. And is consistent with what others have been telling me. I just hope that if we are correct, that I have the power to force them to adhere to these rules.
What can you do if they claim I’m incorrect in saying this, and it’s three against one? I mean the doctor is sort of tied as well, because it’s sort of a social situation: how do you say you want your patient on dialysis three times per week, if the nursing staff says it’s against the rules?
Someone told me to ask the doctor to call the Medicare provider hotline, but I feel like he would not be willing to do that.
And is there no difference in regards to the conventional three times a week regimen as far home versus in facility goes? They keep repeating to me that “home dialysis is meant to be five days per week.”
Either way I appreciate what you’ve been able to come up with. Thank you very very much.
Unfortunately as a dialysis company owner and biller, this is completely related to the the company wanting to bill 4-5 treatments a week. Medicare allows billing up to 5 days a week. In order to be more profitable with your insurance, they do not want to drop to three days a week. Additional the data would support that the Nxstage is not the most appropriate for a 3x a week due to its lower dialysate flow rates. If your goal was 3x a week at home, you could use a full hemodialysis and a marcor RO
I think that last point is more subjective than fact. I mean yea if the machine can’t do the same thing as some other machines in the same amount then because of the fact you have to stay on it longer to reach the same goal then you can say the other ones are better. But if the other ones are not available and if this one still does the job, only it takes an extra hour. Then I personally would rather do dialysis five hours for three days than for two hours for six days. That’s just my personal preference. My last three jobs I worked 12-13 hours a day for three days instead of 8 hours for five days. Because I like having full days off. And an extra three hours in total is minuscule in terms of having four total DAYS off.
And as for the billing thing. They had to give a “example justification” to my doctor in order to give him a way to justify my doing more than three treatments because he couldn’t come up with anything and he just copied it. It’s not like I have any bad labs or I retain fluid. So it just doesn’t make sense that a company can willingly choose to keep a patient on three or more treatments if they don’t need and their doctor specifically orders only three treatments
I don’t want to threaten them with a lawyer. I have an appointment tomorrow with everyone at the center. I will ask them to show proof of what they are claiming and then if they say they don’t have to I will tell them that I have reached out to other sources who tell me they are incorrect and that if they are telling the truth it should be easy to prove. Because my understanding is if the doctor orders it, and my ktv meets standards, there is nothing wrong with it and they have to follow it.
But I feel it’s like dealing with a corrupt cop, who is arresting you and is willing to lie even though you are not breaking the law. They may just continue to deny regardless of the fact that I am allowed to do it. And if my doctor believes them then I have no chance.
Stephen I totally agree with the subjectivity related to using a T machine, you’re exactly correct…just longer slower contact time with the dialysate flows. There are dialysis companies that provide other options than Nxstage at home.
For billing it requires elevated potassium, excess fluid removal in order to justify extra treatments.
This is a problem that you’re describing and what we hope to combat. Let people have the least amount of dialysis needed to let them be happy, healthy, and out of the hospital. Wishing you best on this adventure and feel free to call anytime you have questions or need support for your journey!
Do you have commercial insurance or Medicare. If you have commercial insurance which often pays at least 3 times Medicare’s allowed charge, like Josh says, dialysis clinics like to maximize their profits. The insurance companies (called Medicare Administrative Contractors or MACs) that pay claims filed with Medicare are not consistent in paying for more than 3 treatments. Some do and some don’t but all are supposed to require medical justification to pay for more than 3 treatments a week.
If a patient does 4-6 short daily treatments (typically 2.5-3 hours) using the NxStage machine and your doctor prescribes longer treatments 3 days a week, you could be getting the same or more dialysis 3 times a week as 4-6 daily ones. It is best never to skip 2 days in a row. Dialyzing longer every other day would eliminate that 2 day gap that has been shown to increase the risk of hospitalization and death. MACs seem to not have a problem with that. I’ve heard of patients who have commercial insurance that charges copays for each dialysis treatment and Medicare Part B has a 20% coinsurance for those who don’t have a secondary payer. So if you have commercial insurance with copays or Medicare coinsurance or Medicare denies extra treatments, doing dialysis every other day saves money.
Josh, I found this local coverage determination that was revised in 2020. It includes a lengthy list of codes that could be used to medically justify treatments over 3 weekly. However, it says Medicare won’t pay claims for extra treatments without using one of those codes. https://www.cms.gov/medicare-coverage-database/details/article-details.aspx?articleId=55703
As Josh says, there are other machines that can be used for home HD besides NxStage that your clinic obtain for you. I believe the Tablo is the latest machine approved for home HD.
You also have the option to change clinics to get the treatment that you want. You might have to change doctors.
Correct Beth. They aim for up to five treatments a week with the mentioned codes.
Stephen, you probably are commerical patient, if any company is choosing profits over your needs, safety, switch units. Your doctor would understand and likely has credentialed at other units and companies. You can also report them to the local kidney network. Patient centric, not profitcentric
Stephen, your clinic should have given you information on how to file an internal complaint within your clinic and the corporation that owns if, it applicable. The clinic should have information posted about where to file a complaint with the ESRD Network or State Survey Agency. This Medicare publication gives you information on how to do that.
Here is a map of the U.S. You can put your cursor over your state to get the number of the ESRD Network. If you call, ask for the patient services staff. https://www.esrdncc.org/ESRDNetworkDirectory
According to a nurse friend who worked for NxStage, that machine will provide adequate dialysis with nocturnal dialysis every other night.
The Tablo machine was designed for short daily dialysis, but I don’t think it can do nocturnal and is only FDA-approved for daytime dialysis. The only way any patient can use a Tablo machine is if their clinic gets it for them. I’m not sure how many clinics have ordered Tablo machines for their patients. You might check with Outset Medical to see what clinics are using the Tablo for home dialysis.
There’s another HD machine called Quanta SC+ that has been approved by the FDA for use in chronic (outpatient) or acute (inpatient) facility. The company is in the UK. I don’t know if the SC+ has been approved for home use. You can see the machine and contact the company from this site. https://www.quantadt.com/
Oh thank you very much for following up! Well during the visit they said it would not be possible now no longer cause of reimbursement but because I am using hanging bags and they would not allow me to use so many bags on the IV pole, or change them out mid treatment(the connectors only hold so many.) Then I said I will go back to using pureflow and they said that it doesn’t matter because it’s fresenius policy not to allow nxstage patients to do it three times per week. So I questioned them about their policies and asked them how could I even remain their patient if that is the case considering it requires medical justification to get reimbursement for more than three treatments per week and according to my doctor and I, and the local determination for coverage, I don’t meet any of the valid reasons. I don’t have fluid problems, I have a lot of residual function, and my labs are great and I met adequacy just fine in center. It’s not according to my wishes I want to leave you guys now, it’s according to your own policy. Then they sent me this twenty four hours later.
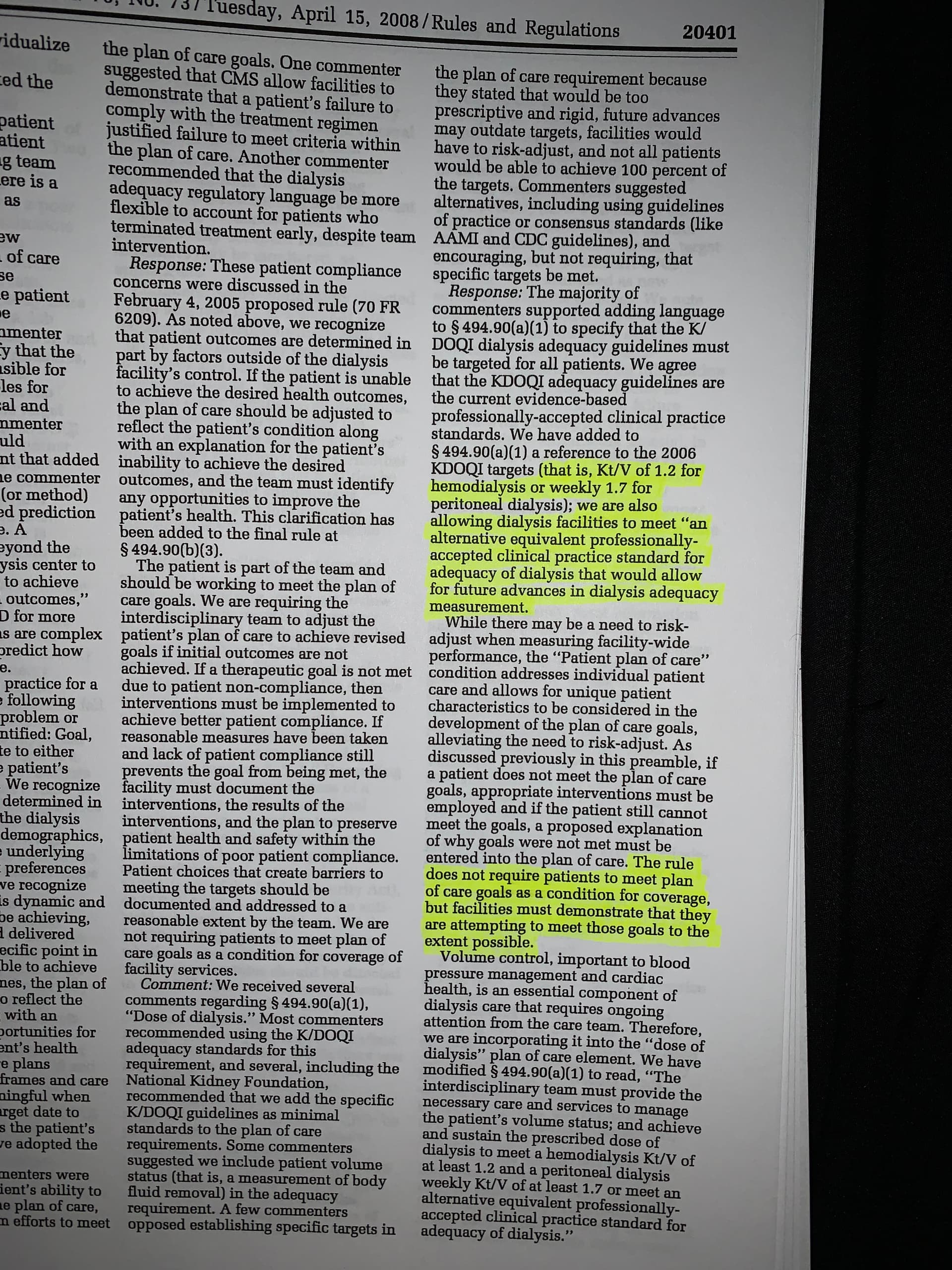
But I was researching a lot before this appointment (you guys were a big help thank you kindly) and I found this in the conditions for coverage
(I will post it in another reply)
So now I am going in there again to discuss this hanging bag dilemma because over the phone they told me I will have to have a partner and meet ktv, or I will be forced to go back to more treatments. I consider this hanging bag issue a complete lie as I see now how the Medicare excuse was. I contacted another clinic and they said that whatever the doctor prescribes is what my treatment frequency will be, and that they see no problem with the hanging bags being put on mid treatment. I’m going to do more research on the ktv target and if it is really required for reimbursement (I have a contact in the esrd division in cms now, they are very nice they actually responded to me very promptly after emailing them.) And also I’m gonna tell them if they keep trying to pursue this fight to get me back to more treatments I am done with them.
And I will be sure to keep you posted. But that’s all the information for now.
I should mention that this is a big success and when I used your name Beth was able to instantly win over the support of my social worker, a big thank you to you specifically, thank you so very much.
Hi Steven. When I first read your reply, I was perplexed about why your clinic would require a partner for 3x/week home HD. It took me half a moment to realize that this makes sense–and coincides with why I would strongly recommend that you consider every other day treatments instead of just 3x/week.
You said, “I don’t have fluid problems, I have a lot of residual function, and my labs are great and I met adequacy just fine in center.” Awesome. You want to keep that residual function. Every mL of residual function you keep extends your life. The thing that is most likely to reduce your residual function is doing dialysis only 3 days a week, IF that means you STUN your heart, brain, gut, and any kidney function you have left by having to pull fluid too quickly or pull too much to get to your goal. The more urine you still make, the less likely this is–but that will drop over time.
I wonder if doing every other day treatments would let you keep doing solo, since the risk of a “crash” (drop in blood pressure – organ stunning) is so much less without a 2-gap? That might be worth asking if you don’t have someone who can be a partner. (Keep in mind that in those same Conditions for Coverage, Medicare NEVER defines the role of a “care partner” or “caregiver.” So, just having someone in the home who could call 911 if you crash could be enough.) But, most clinics will want to train a care partner to at least stop the machine. And, some go overboard and try to turn care partners into technicians, even for people who are perfectly capable of doing their own treatments.
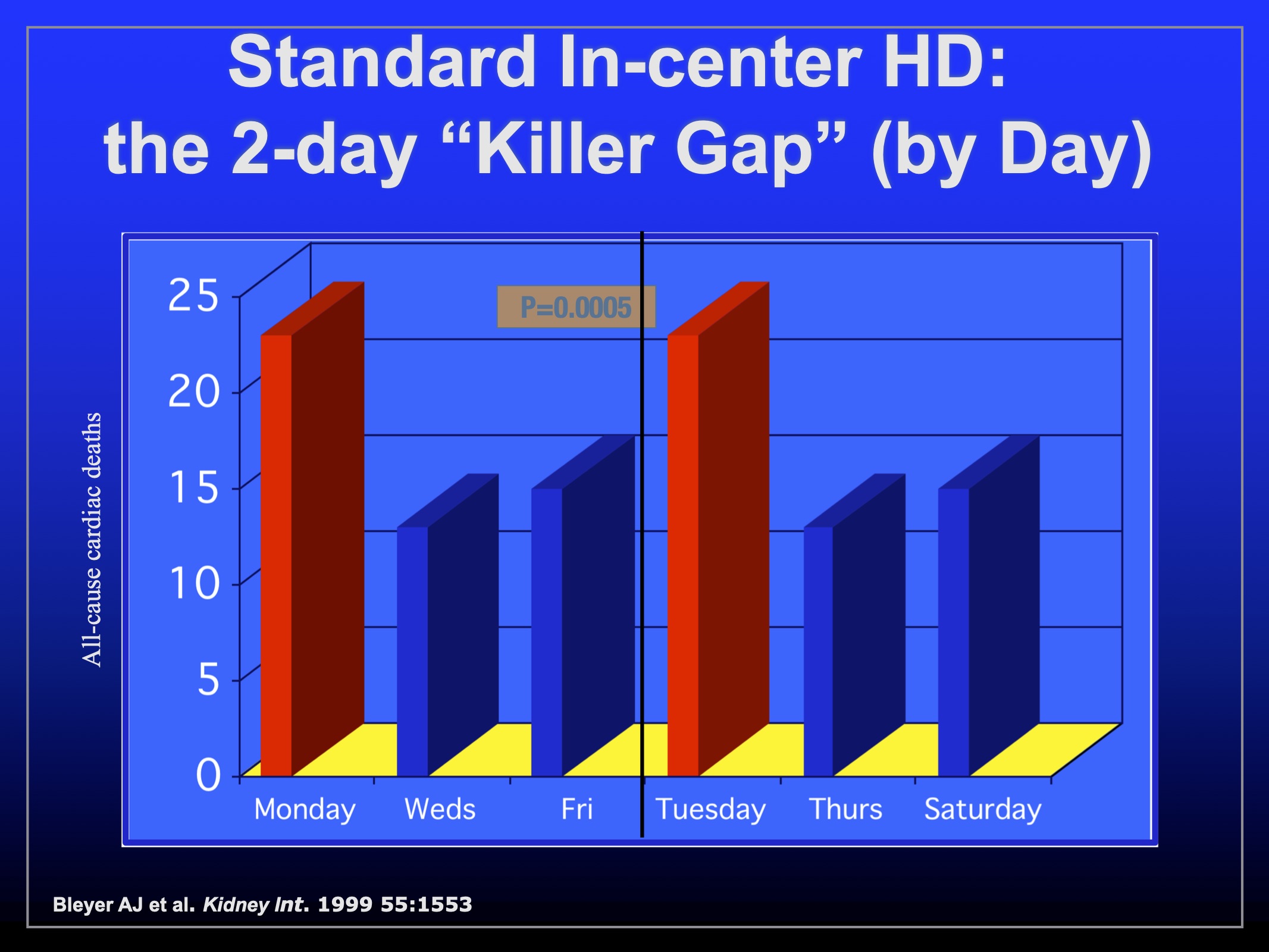
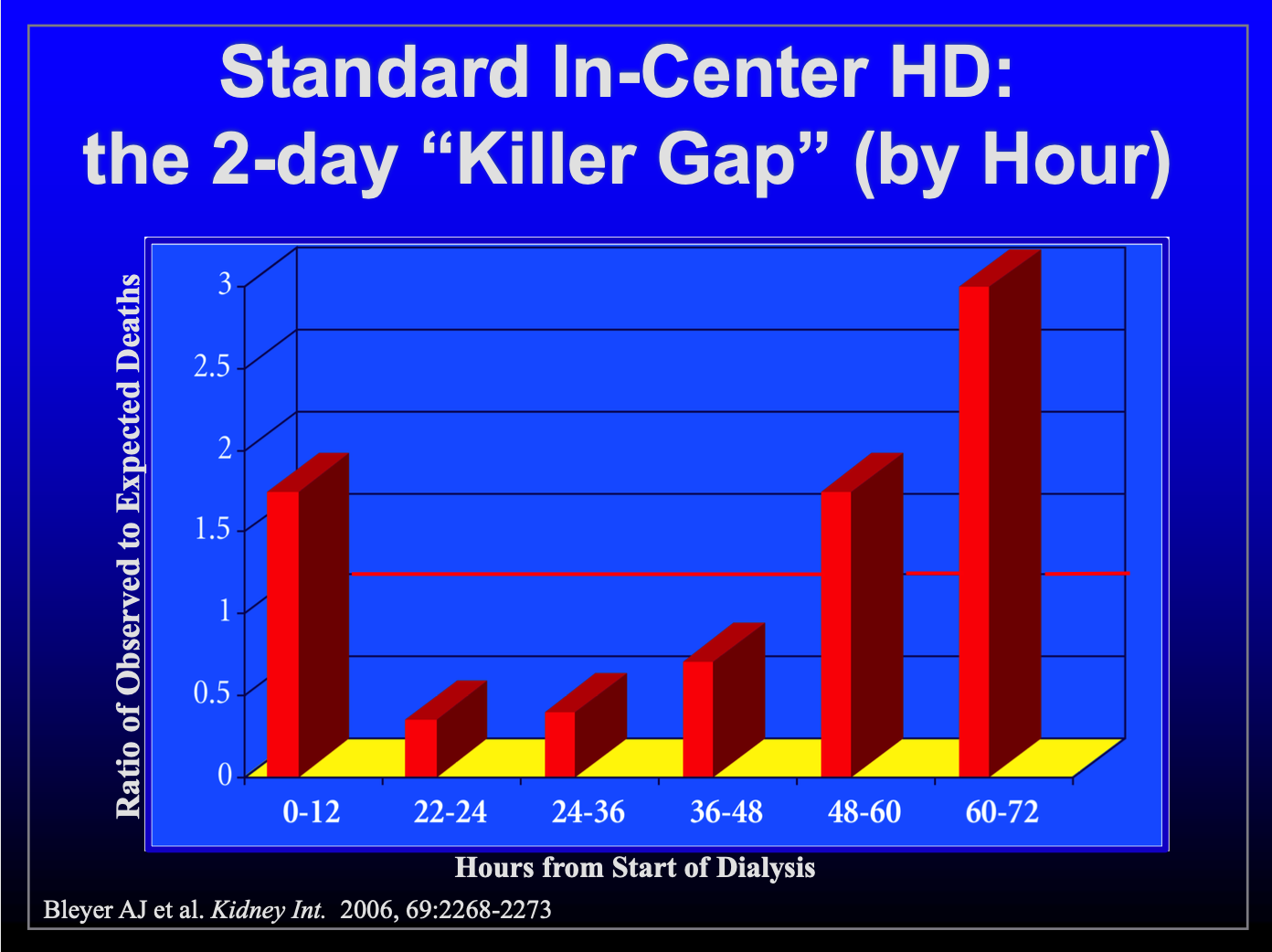
My very strong personal bias, which is based on population research with hundreds of thousands of people on dialysis, is to never have a 2-day gap, and never do aggressive ultrafiltration. Not to get too morbid on you, but people on peritoneal dialysis have an equal chance of dying on any of the 7 days of the week. This is not true with standard HD. Folks who did that were 50% more likely to die on a Monday or Tuesday after the 2-day no-treatment weekend. And, in the 12 hours before that Monday or Tuesday treatment, the risk of death was triple.
If every other day will fit your life, maybe think about it and see if you could do that solo? Another option, if you don’t travel, may be to ask your clinic to train you on a full-sized Fresenius machine.
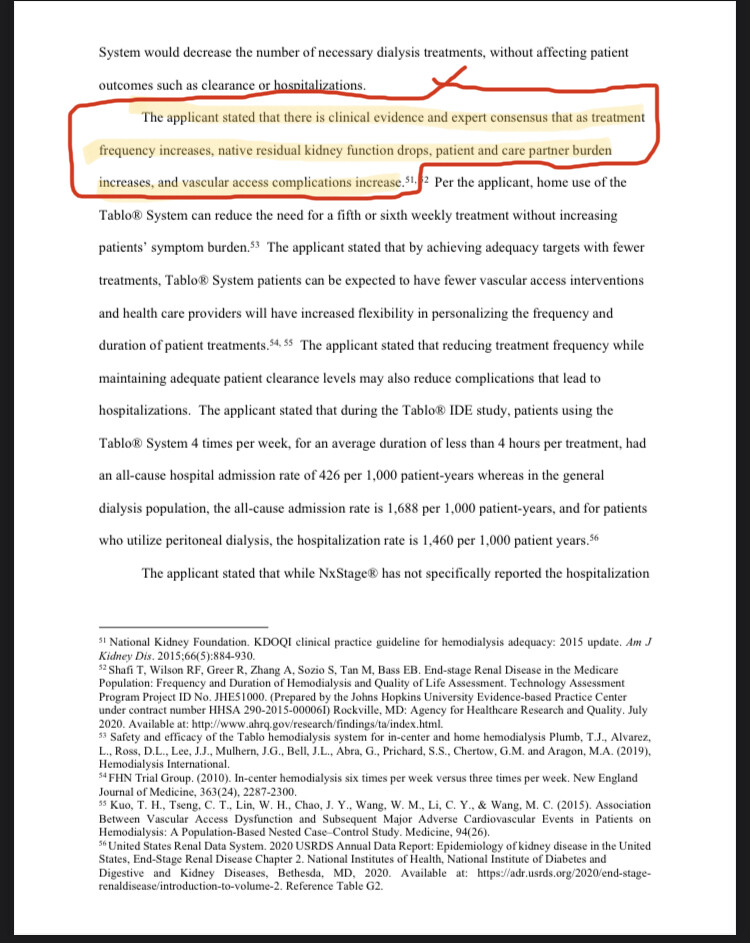
I like this fact I am aware of it. I bring it up every holiday because sometimes their scheduler puts two two day gaps four days apart two weeks in a row and I’m like what are you doing ?? I forgot to mention I do not remove fluid. Not even the rinseback. It’s so hard to remember what is significant and worth mentioning when it is so difficult to pretend to not know what you already actually know. I don’t remove fluid and it’s been that way for years. And I read that if you increase dialysis frequency then your residual kidney function drops. This is the 2022 proposal rule changes for cms and hhs, it’s 345 pages long with tons if facts and every page has citations:
Most employers do not offer a full time position working every other day. And to me, having those weekends are a big deal for my mental health. Not having more than one day off for years to come? That sounds terrible I would rather do three long treatments and have four normal days with one weekend per week. Then five short treatments per week with no weekend. I will strive for this until the very end. Quality of life is number one for me, above all else. I am not equipped to go in center and do dialysis all week I just can’t I’m sorry
I wasn’t talking about doing in-center–I meant doing every other day at home, where you can decide when you want to do the treatments. It’s not the number of days that affects residual function–it’s how aggressive the water removal is. Right now, there’s none, and you are just removing toxins. That should work 3x/week, while your residual lasts. The challenge is that you need a partner to do that at home. Do you have one?
Sorry I am a poor communicator. I don’t have anyone who can help me. Outside of my part time job I am a recluse. My mother is the only person who can help me but she is a manager and she works five am to six pm Monday through Saturday and I don’t want to coordinate my life around here especially because I think these nurses are coming from bad intentions.
My prescription currently is 50L 4hr 30min every other day on nxstage at home hd. I can’t do in center as a way to do three times per week which I know you are not saying but others outside of this forum have suggested. And I cannot do without the two day breaks. I can’t handle working with other people (and plus the turnover in centers in my area have been very high anyway so just as you’re getting to establish a way of working with eachother they are changed for new staff.)
And my issues with this care partner stuff is it is not genuinely about patient safety, the connectors only hold 40L and I have to change bags mid treatment CURRENTLY(and I have been on this prescription for six months) so essentially the process for 60L would be the same only a quantity of four bags being changed instead of the current two bags being changed.
Also their excuses went like this x>It’s Medicare reimbursement>y>We don’t want you changing bags mid treatment alone>z>it’s company policy! So why start with these five other reasons if the whole time the reason was company policy? Did they not know it was company policy for the past four months I’ve been asking until somebody filled them in this past week?
And also why did I get approved twenty four hours after I asked to see the policy on paper and I mentioned that prohibiting patients from doing three treatments at home while Medicare prohibits more than three without medical justification means that anyone who doesn’t require the more treatments shouldn’t be at home at all when in fact home dialysis is sold to patients on the basis that you get independence?
Their logic just contradicts itself and that is because they are not behaving based on patient centered treatment they are profiteering the whole way through and nothing they say should be considered a neutrally objective observation/suggestion to help me, if attached to the suggestion is the requirement to move back onto more treatments. Especially since “coincidentally” they get paid more for me doing more treatments. This to me is blatant malice and profiteering, not patient safety.
The more I think about this the more I think I should change doctors as well. Because he approves me for everything I want(but I think that has more to do with the fact that what I ask for is always reasonable and he is not motivated by money). But he should shift his tone with this staff and start questioning them now that they have proven that they aren’t being direct with me and that they have other motives. Not to give in to their demands so easily.
And he’s either doing that because he doesn’t see them the way I do, or he sees what I’m seeing and he just doesn’t want to get into confrontation. But either way I have a problem with that because what that means in practicality, is I have had to advocate for myself all alone and it has been one SERIOUS struggle.
I don’t think you are a poor communicator! And, I’m sorry that advocating for yourself has been such a struggle. Systems are set up to benefit the folks who set them up, not those who have to live within their constraints.
 what you’ve been able to come up with. Thank you very very much.
what you’ve been able to come up with. Thank you very very much.
 Then I said I will go back to using pureflow and they said that it doesn’t matter because it’s fresenius policy not to allow nxstage patients to do it three times per week. So I questioned them about their policies and asked them how could I even remain their patient if that is the case considering it requires medical justification to get reimbursement for more than three treatments per week and according to my doctor and I, and the local determination for coverage, I don’t meet any of the valid reasons. I don’t have fluid problems, I have a lot of residual function, and my labs are great and I met adequacy just fine in center. It’s not according to my wishes I want to leave you guys now, it’s according to your own policy. Then they sent me this twenty four hours later.
Then I said I will go back to using pureflow and they said that it doesn’t matter because it’s fresenius policy not to allow nxstage patients to do it three times per week. So I questioned them about their policies and asked them how could I even remain their patient if that is the case considering it requires medical justification to get reimbursement for more than three treatments per week and according to my doctor and I, and the local determination for coverage, I don’t meet any of the valid reasons. I don’t have fluid problems, I have a lot of residual function, and my labs are great and I met adequacy just fine in center. It’s not according to my wishes I want to leave you guys now, it’s according to your own policy. Then they sent me this twenty four hours later.
 I would rather do three long treatments and have four normal days with one weekend per week. Then five short treatments per week with no weekend. I will strive for this until the very end. Quality of life is number one for me, above all else. I am not equipped to go in center and do dialysis all week I just can’t I’m sorry
I would rather do three long treatments and have four normal days with one weekend per week. Then five short treatments per week with no weekend. I will strive for this until the very end. Quality of life is number one for me, above all else. I am not equipped to go in center and do dialysis all week I just can’t I’m sorry 