Dr. Agar,
I was wondering what Australia’s clinics have for patient/staff ratios? Here I’ve heard good staff ratios would be 9 patients for 3 techs and 1 nurse. Do you even use techs there?
Thanks!
Dr. Agar,
I was wondering what Australia’s clinics have for patient/staff ratios? Here I’ve heard good staff ratios would be 9 patients for 3 techs and 1 nurse. Do you even use techs there?
Thanks!
In Australia, almost all dialysis is administered, supervised, provided, and hands-on-delivered by dialysis-trained registered nurses (RN) – a significant proportion (41%) of whom have completed a course in advanced dialysis theory and practice. In some units (like my own) this percentage is very much higher as (we) encourage all our nurses to complete additional training and have self-funded this training from within the units’ state-provided budget. As an ‘aside’ here, we have managed to do this from the savings we have managed to accrue from our home hemodialysis program where, as you know, +/- 30% of our HD patients self-dialyse at home on long slow, overnight dialysis which is, in our view and our experience, both better (in clinical otcome) and cheaper (in program cost) than facility-based care.
Paul Bennet reviewed Australian and New Zealand dialysis nursing practice in 2009. You will see from his paper …
http://dspace.flinders.edu.au/jspui/bitstream/2328/26260/1/Bennett%20Australian.pdf
… and especially from Figure 2 and Figure 3 … that the data varies, state to state, with some states (eg: Tasmania) being entirely dialysis-trained RN dependent, to South Australia where a little over 20% of staff are not registered nurses but are state enrolled nurses (SEN) = full-time nurses who have been trained to diploma level. Figure 3, however, shows that a significant % of renal SEN’s have also completed renal higher education courses.
RNs (= the vast bulk of all dialysis-administering personel in ANZ) are, on the other hand, university qualified nurses who have successfully completed both a university tertiary degree in nursing and general training, most commonly in teaching hospital settings.
You will likely find more information in his paper. I would suggest you read it rather than for me try to paraphrase it here.
Dialysis technicians are not widely encouraged or broadly supported either. Their use in some hospital programs comes largely as a ‘grandfathered’ anomaly from the dialysis programs of the 60s and, despite some strong opposition at times from the nursing bodies, has persisted – generally in individual institutions – against the national norm.
As for staffing levels, the national ratio – again varying from state to state (but only marginally so) – is currently set at 1 x dialysis-trained RN for every 3.5 x patients in satellite dialysis facilities (lower-acuity care) while in-centre facilities (higher acuity care) generally run a 1 x dialysis-trained RN to every 2 x patients.
This can be seen in a recent re-positioning document from Kidney Health Australia – a document that has developed the model for and makes national recommendations on, among other things, home dialysis …
http://www.kidney.org.au/LinkClick.aspx?fileticket=BfYeuFvtJcI=&tabid=811&mid=1886
KHA is the Australian ‘equivalent’ for the NKF in the US … and as a potential ‘conflict of interest, I have both recently stepped down from the Board of KHA after my alloted period of ‘tenure’ and have been intimately involved with the development of the model through my founding membership of the Home Dialysis Advisory Group … a subcommittee of the ANZSN (Australian and New Zealand Society of Nephrology).
Page 14 of this document references the mean national staffing ratios.
I hope this has been of some help.
This has been a great help! I recall going through the USRDS stats here and finding how much we are spending per patient overall. You wouldn’t happen to know where I might find something similar for Australia?
Dear Plugger
Perhaps I should just write a book for you on Australian dialysis and be done with it!
But - only poking fun … so, here goes …
While dialysis costs have long been assessed and reported – one of the first in the literature reports being our own …
Agar JWM, Knight RJ, Simmonds RE, Boddington JM, Waldron CM, Somerville CA. Nocturnal Haemodialysis: An Australian cost comparison with conventional satellite haemodialysis. Nephrology (Carlton) 10(6): 557-570 December 2005
To my knowledge, this paper along with Phil McFarlane’s similar and roughly coincident report from Canada, were the first detailed reports of the cost advantages of home dialysis … and remember, than in our report, we compared 6 x hrs/week home HD with 3 x 4hrs/week low acuity facility-based care (in Australian parlance = satellite HD) - yet the home HD option still cost significantly less! I will leave it to you to source the McFarlane paper from Canada.
Now … this is important … there are a number of problems with and pitfalls in ‘cost’ reporting - any cost reporting.
The most important of these is to know what is actually being compared or reported in each attempt at cost-assessment … ie: what is sometimes referred to as the ‘apples-with-apples’ or ‘apples-with-oranges’ comparison conundrum.
Some reports simply list the consumable costs of dialysis: the fluids, the lines, the on-off packs, etc … the day-to-day expenditure of the process itself – yet even these often leave out things like the provision of ultra-pure water (the costs of water management), the costs of power. Other reports add in (variously) medications, pathology, radiology, ancillary care (dietetics, physio, OT, etc.) doctors visits, travel, and public transport costs, lost time from work, social security supports, hospitalizations + the in-hospital costs of those hospitalizations … the list goes on. Then there are the machine costs + insurance + depreciation, there are the building and infrastructure expenses and staffing wages.
The list is almost endless and every costing study I have read – and that’s many – adds or excludes some (or many) of these.
So … to get a good idea of what dialysis costs almost becomes meaningless, as, in the final analysis, the per person per year costs become mind-bogglingly large! Here, In Australia, the current cost being bandied about (and I think it is not far from the mark as a TOTAL ALL UP cost per person per year AND where on current rates of trade $1 Australian equates to $1.05 US) boils down to
[B]· Hospital Haemodialysis = $79,072 …. equates to high acuity haemodialysis
· Satellite Haemodialysis = $65,315 …. equates to low acuity haemodialysis
· Home Haemodialysis = $49,137
· Peritoneal Dialysis = $53,112[/B]
For the reference to this … see
Now … that said, there is a more detailed analysis under the heading ‘Economic Impact of the Burden of ESKD in Australia - Projections to 2020’ = available at:
http://www.kidney.org.au/HealthProfessionals/CKDinAustralia/tabid/622/Default.aspx
How these relate to costs elsewhere is debatable. Machines are imported here – as are many of the trappings that go with them. This implies import costs. The wage structures are different, the working hours and overtime arrangements differ. Almost any or every part of the chain differs … so how this can be sorted – one country with another – is almost impossible to dissect and quantify.
One thing that I think is (likely) valid … and that is that the differential costs between modalities will hold true – across borders and across systems.
Facility-provided dialysis is always going to be the most expensive. If you ‘average’ the costs of facility dialysis using a ¼ (high acuity) vs. ¾ (low acuity) ratio (= roughly a true estimate of the high vs. low acuity spread), then the mean cost of facility dialysis on these data = Au$68,754.
Oh … and, incidentally, it is the low acuity ‘satellite’ patients who are, in the main, potentially home-capable.
This means that home-based HD is roughly Au$20,000 per patient per year (or 71%) of the ‘averaged’ cost of any form of facility-based HD care. Draw your own conclusions – especially if you remember that it is the home dialysis patients who also have the better outcomes!
But … did I forget to mention that the home HD patients also live twice as long? … see
Marshall MR, Hawley CM, Kerr PG, Polkinghorne KR, Marshall RJ, Agar JWM, McDonald SP. The effect of home haemodialysis on mortality risk in Australian and New Zealand populations. Am J Kid Dis. 58(5): 782-793. August 2011.
So … perhaps the cynic in me says that in the long run, home dialysis patients might cost more – in dialysis costs – than facility-based patients who only survive half the time.
But, then again, most of our home dialysis patients (or at least those of working age) are in work. So, they are tax payers … and, by and large, they do not draw social security pensions or payments!
… and so the argument goes on …
There – much of your work has now been done for you!
Thanks once again!! And if you write that book on Australian dialysis I will buy the first copy!
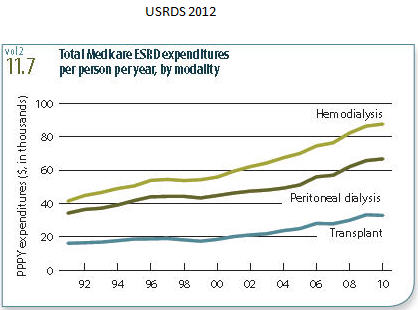
I did look up what Medicare pays per year for per patient costs: $87,561US for hemodialysis. I also updated a graph I have for US costs over the years: http://dialysisethics2.org/open_images/per_patient_cost.jpg.
So believe your country is paying $68,754AUS ($72,192US) per person for facility hemodialysis, compared to our $87,561US! -for bazooka-style dialysis.
Guess Kent Thiry’s circus act has been very successful keeping our politicians distracted: http://www.5280.com/magazine/2012/09/strangest-show-earth
Dear Plugger
While on the face of it, that seems possible, I again caution you that
(1) I am only quoting the Australian data from KHA (see the KHA link in the previous responses). While it emanates from The George Institute, one of (if not THE) most prestigious Australian health economics research groups from Sydney … and they certainly do their stuff meticulously - I cannot confirm exactly what is or is not IN (or OUT of) their costings. I suspect the same may be said for the source of your US data too.
(2) it is absolutely vital - I made this point in my original posting on this issue - that each costing is comparing exactly the same data points. Do they, for instance, include or exclude pathology, inpatient care, radiology, clinic visit costs, ancillary care … etc etc.
Be cautious on this … for direct comparisons can be fraught with misinterpretations -and thus off-the-mark conclusions.
Then … worse … if you USE the costing information and it proves to be apples with oranges and NOT apples with apples, not only may you end up with egg on your face, but the funding sources themselves (while quite above board and accurate in their own right) may also suffer from any ill-measured use of their information.
I’ll heed your warning, I’m calling what we have preliminary data. And if all else fails, there is this about the Italians:
“Italy has one of the lowest mortality rates for dialysis care – about one in nine patients dies each year, compared with one in five here. Yet Italy spends about one-third less than we (in the U.S.) do per patient.”
{kind=link}